





Introduction
Penile implant surgery remains a gold-standard treatment for men with end-stage erectile dysfunction (ED) unresponsive to pharmacological or less invasive therapies. Despite its efficacy, complications can occur, with cross-over being a relatively rare but challenging issue to manage. This case report focuses on a 45-year-old diabetic male who presented with a distal cross-over after undergoing a malleable penile implant procedure using the Tube Promedon device. We discuss the clinical presentation, diagnostic evaluation, surgical management, and review the current literature on this complication. The aim is to provide insights into the prevention, diagnosis, and treatment of cross-over to enhance surgical outcomes.
Case Report
A 45-year-old male with a history of diabetes mellitus and end-stage ED was referred for persistent glans pain and a twisted penile implant. Six months prior, he had undergone malleable penile implant surgery with a Tube Promedon device at another center. The patient reported continuous discomfort localized to the glans, which had persisted since the surgery. Physical examination revealed that the left side of the glans was empty, while both rods of the implant were palpated in the right side of the glans. The implant also exhibited a twisted configuration, consistent with a distal cross-over.
Diagnostic Imaging
To confirm the diagnosis, an X-ray of the penis and MRI were performed. The imaging studies revealed that both hinges of the malleable implant had crossed over to the right side of the glans, with no rod present in the left glans. These findings corroborated the clinical suspicion of a distal cross-over.
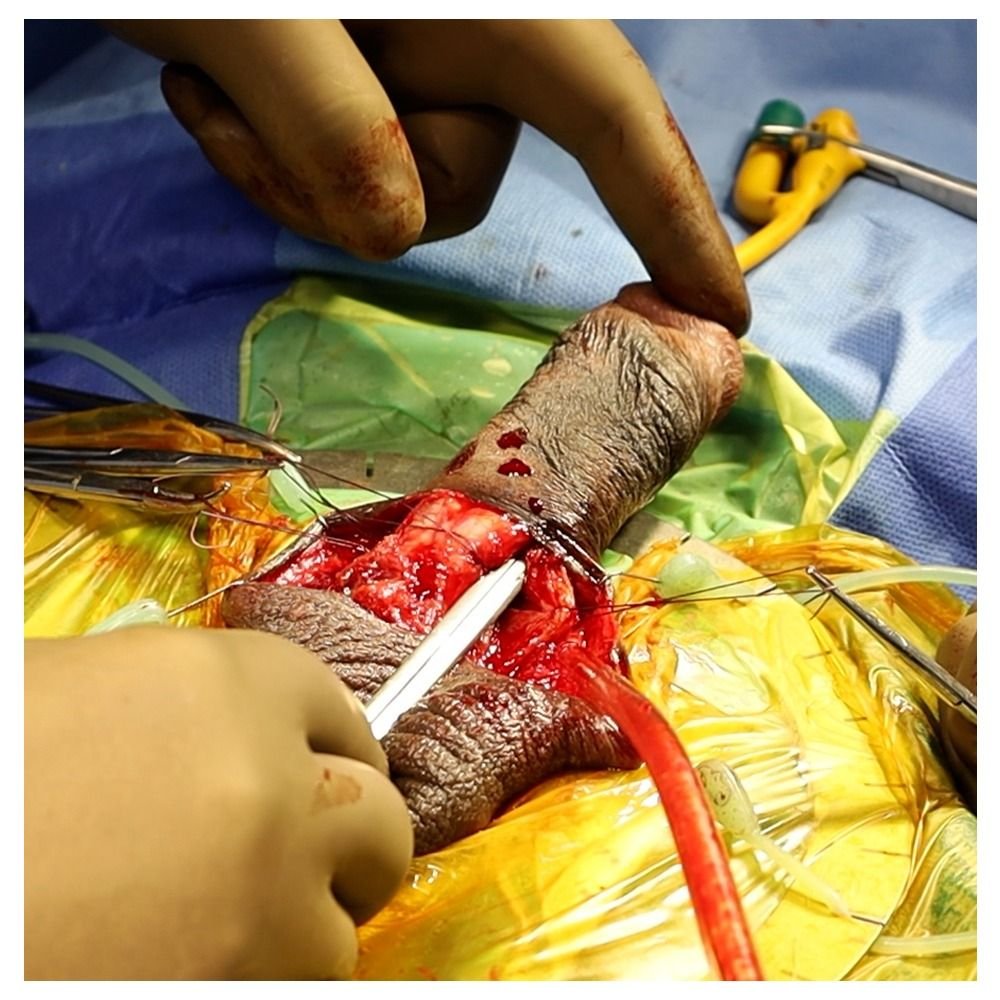
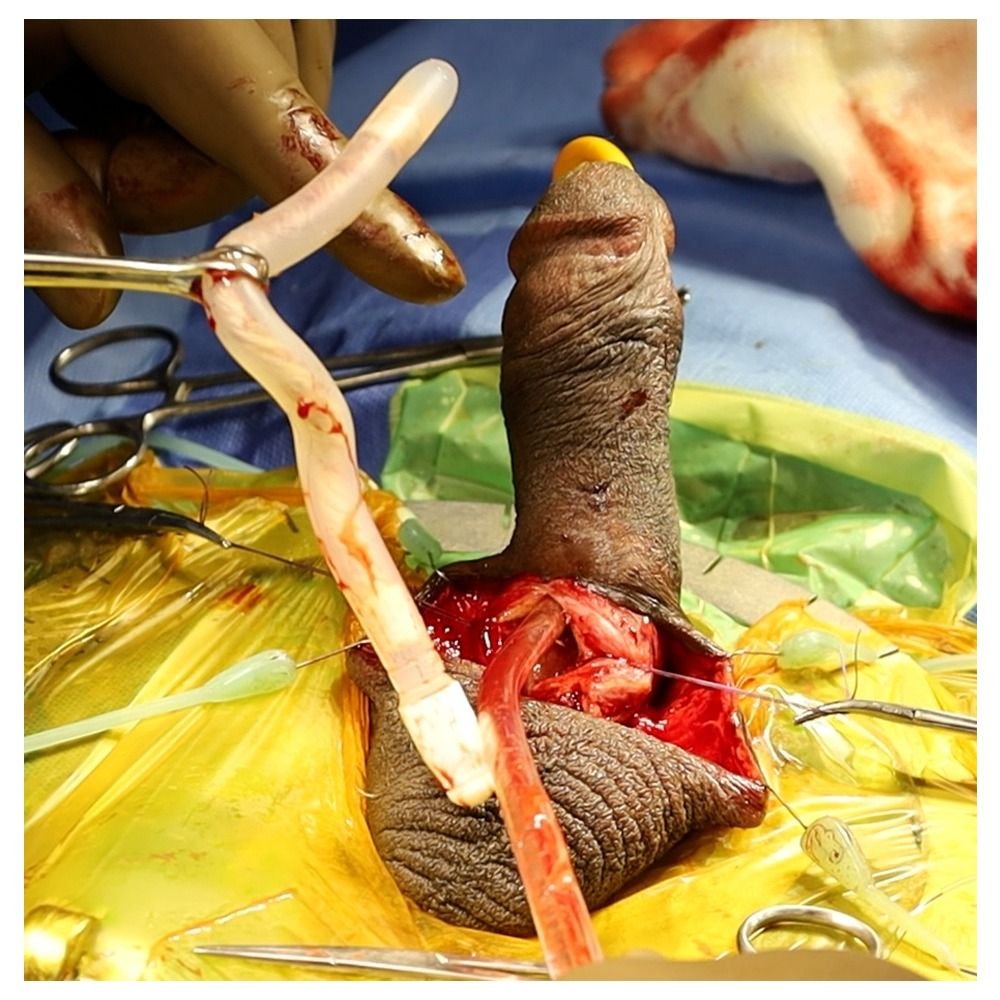
Surgical Revision
Given the significant discomfort and dysfunction associated with the cross-over, a revision surgery was planned. The surgical approach involved the removal of the misplaced rods, redilating the crura, and placing a fresh implant. During the revision, the surgical team utilized several preventative techniques to avoid reoccurrence of the cross-over, including the goalpost test and careful crural dilation. Post-operative recovery was uneventful, and the patient reported significant relief from pain and restored function at his follow-up appointments.
Discussion
Penile implants have significantly improved the quality of life for men with refractory ED, but surgical complications remain a concern. Cross-over, wherein one or both rods of the implant migrate across the midline into the contralateral corpus cavernosum, is an uncommon but well-documented complication. Although most commonly described in inflatable penile prosthesis (IPP) surgery, cross-over can also occur in malleable implant procedures, as demonstrated in this case.
Etiology of Cross-Over
Several factors may contribute to the occurrence of cross-over during penile implant surgery:
1. Absence of a Foley catheter: The lack of a Foley catheter to stabilize the penis during surgery can lead to inadequate control of the penile position, increasing the risk of cross-over during dilatation of the crura.
2. Insufficient penile stretching: Inadequate stretching of the penis during crural dilatation can prevent symmetrical placement of the rods, resulting in cross-over.
3. Peyronie’s disease: The presence of fibrotic plaques in Peyronie’s disease can distort the normal anatomy of the penis, making it more susceptible to cross-over during implant placement.
4. Thin septum: Some patients may have a congenitally thin septum, making it easier for the dilator or implant to breach the midline and cross over to the contralateral side.
5. Aging and senile changes: In older men, age-related thinning of penile tissues can compromise the structural integrity of the septum, facilitating cross-over during surgery.
Prevention Strategies
To prevent cross-over, several intraoperative techniques have been described in the literature:
1. Goalpost test: The goalpost test is a simple but effective maneuver used after dilating the crura. By placing two instruments in each crus and aligning them, the surgeon can confirm that both crura have been adequately dilated and that cross-over has not occurred. If the instruments do not align, the surgeon must correct the misplacement before proceeding with the implant.
2. Sequential dilatation: If cross-over is suspected during surgery, placing a dilator in one correct crus while redilating the contralateral crus can prevent further misplacement. This ensures that both crura are adequately dilated and separated.
3. Use of a Foley catheter: The placement of a Foley catheter during surgery can help stabilize the penis and prevent rotational movement during dilatation, reducing the risk of cross-over.
4. Preoperative assessment: Careful preoperative assessment, particularly in patients with Peyronie’s disease or thin septa, can help identify those at higher risk for cross-over. In such cases, surgical planning can be adjusted to mitigate these risks.
Review of Literature
Although cross-over is a well-recognized complication of penile implant surgery, its exact incidence is difficult to determine due to the variability in reporting. Most studies report cross-over rates ranging from 1% to 5%, with higher rates observed in revision surgeries and patients with anatomical abnormalities, such as Peyronie’s disease.
In a review of 150 penile implant cases, Mulcahy et al. (2004) reported a 3% incidence of cross-over in malleable implants, which was higher than the 1% incidence observed in inflatable devices. The authors attributed this difference to the more rigid nature of malleable implants, which can make crural dilatation more challenging, particularly in patients with abnormal penile anatomy.
Henry et al. (2015) reviewed the outcomes of revision surgeries for penile implants and found that cross-over was a common reason for reoperation. In their cohort, 4% of patients required revision due to cross-over, with most cases occurring in malleable implant surgeries. The authors emphasized the importance of intraoperative techniques, such as the goalpost test, in reducing the incidence of this complication.
Other studies have highlighted the role of patient selection in preventing cross-over. Chung et al. (2018) noted that patients with Peyronie’s disease, a thin septum, or a history of previous penile surgery were at higher risk for cross-over. The authors recommended preoperative imaging and meticulous surgical technique to minimize this risk.
Management of Cross-Over
The management of cross-over typically involves revision surgery, as was the case with our patient. During revision, the misplaced rods must be removed, and the crura redilated before placing a new implant. Some surgeons advocate for the use of a different implant type (e.g., switching from a malleable to an inflatable implant) during revision to reduce the risk of reoccurrence, particularly in patients with Peyronie’s disease or other anatomical abnormalities.
Intraoperative imaging, such as fluoroscopy or ultrasound, can be helpful in confirming the correct placement of the rods during revision surgery. However, these modalities are not routinely used and are typically reserved for complex cases.
Outcomes and Prognosis
When appropriately managed, the prognosis for patients with cross-over is generally good. Most patients experience significant improvement in pain and function following revision surgery. However, patients with underlying conditions, such as Peyronie’s disease or significant penile fibrosis, may be at higher risk for recurrence of cross-over or other complications.
In our case, the patient experienced complete resolution of pain and restored penile function after revision surgery. He continues to be followed in our clinic, with no evidence of recurrent cross-over at his most recent follow-up visit.
Conclusion
Cross-over is an uncommon but significant complication of penile implant surgery, particularly in patients with predisposing factors such as Peyronie’s disease, a thin septum, or previous penile surgery. Careful surgical technique, including the use of the goalpost test and adequate penile stretching during dilatation, can help prevent this complication. When cross-over does occur, prompt diagnosis and revision surgery are essential to restore function and alleviate pain.
Further research is needed to better understand the risk factors for cross-over and to develop strategies for reducing its incidence. In the meantime, surgeons should remain vigilant for this complication and be prepared to manage it effectively when it arises.
References
1. Mulcahy JJ, Carson CC, Wilson SK. Penile implant surgery: A review of 150 cases. J Urol. 2004;171(2):549-552.
2. Henry GD, Karpman E, Brant W, et al. Revision surgery for penile implant complications. J Sex Med. 2015;12(5):931-936.
3. Chung E, Ralph D, Karpman E. Predictors of mechanical failure and clinical outcomes after penile prosthesis implantation. J Urol. 2018;199(5):120-126.

