Surgery For Obstructive Azoospermia In
New Delhi India
Welcome to New Delhi India. Dr Vijayant G Gupta is the Foremost expert in performing micro surgery for obstructive azoospermia in this part of the world. He regularly performs Microsurgical Vasoepidydmostomy (VEA or Vaso Epidydmal Anastomosis) by the Single Suture Double arm needle Longitudinal Instussusception technique (Also called Microsurgical LIVE technique for Azoospermia).
He performs more than 100 cases a year and is the highest volume center for this indication in India. His patency rates are 64 percent at 1 year with pregnancy rates of 35 percent (including assisted reproduction).
He is an active member of the International Society of Sexual Medicine and European Association of Urology. Besides numerous publications in National and International journals, he also provides training to visiting Surgeons worldwide. He is an expert in managing male infertility.
What Is Obstructive Azoospermia?
Obstructive azoospermia means the absence of sperms in the semen due to blockage.
Obstruction can be at many levels in the genital tract. The blockage can be at the level of the
- Testis head – Rete testis aplasia
- Epidydmal tubules
- Vaso Epidydmis junction
- Absence or fibrosis of vas
- Seminal vesicle obstruction
- Ejaculatory duct obstruction
- Prostatic cysts
Obstruction can be primary or congenital. It can also be secondary to infections and surgery. Vasectomy is a secondary cause of azoospermia and may require a vasectomy reversal.
What Are The Surgical Options For Treating Obstructive Azoospermia?
Once we confirm that there are live mature sperms in the testis, a thorough search is made for the level of obstruction. Depending on the level and cause of blockage, the surgical options include
- Vasectomy Reversal – In men with prior vasectomy
- VEA or Vasoepidydmal Anastomosis (AKA Microsurgical Vasal Anastomosis (MVA) or Vasoepidymostomy
- TURED or Transurethral resection of Ejaculatory duct
What Is Microsurgical Correction of Obstructive Azoospermia? (Live / Vea / Vasoepidydmostomy)
If the blocakge is at the level of the testis head or the epidydmis, then these obstructions can be bypassed. The surgery to bypass the obstruction is called VEA or Vaso Epidydmal Anastomosis.
The surgical techniques for this has gone through several modifications. Currently LIVE or Single Suture Double arm needle Longitudinal Instussusception technique is the most successful technique for this diffcult surgery.
In this the patent vas is disengaged from the blocked portion, flushed and then joined to a healthy tubule in the epidydmis.
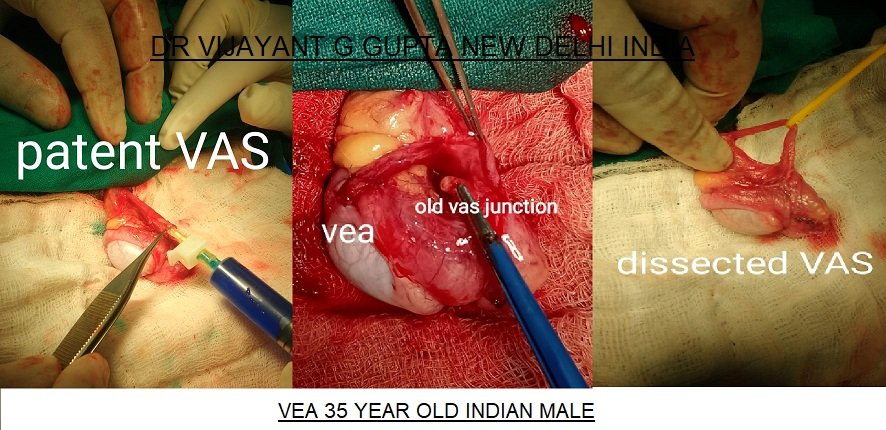
What Are The Surgical Steps Of Vasoepidydmostomy / Live Technique (Vaso Epidydmal Anastomosis) ?
The surgical steps are as follows.
The testis is delivered out under sterile conditions. The vas is dissected and disconnected from the vaso – epidydmis junction. The vas is flushed to confirm patency. The junction is flushed and aspirated to confirm no sperms are present.
Then the epidydmis is assessed. The blocked portion is identified either in the caput or the tail. Usually identification is done under magnification and with sperm aspiration under a microscope.
The epidydmis opened and healthy epidydmis tubules selected for anastomosis.
Using a double armed nylon 10 – 0 suture, LIVE technique is used to intussusscept the tubule inside the vas.
The entire surgery is performed under very high magnification and requires extreme level of training to achieve a successful result.



What Are The Success Rates of Microsurgical Treatment Of Obstructive Azoospermia ?
The success rates depend on 6 important factors. They are
- Age of patient – Younger the better
- Testis condition – Testosterone, FSH and Testis size
- Sperm aspiration from tubule – Finding sperms in the tubule
- Vasal Patency and vasography findings
- Quality of surgery – Technique used, Surgeon Experience
- Presence of past infection or epidydmitis
If all factors are good, then success rates can be as high as 75%.
My success rates are (Year 2017 and 2018, Total patients 209, Follow up atleast 6 months)
- Sperm positivity rate at 3 months – 34% and at 6 months 64%
- Normal sperm count (more than 15 million) – 25% at 3 months and 45% at 6 months.
- Pregnancy rate (Spontaneous pregnancy) – 15% (With IUI) +12% (With ART) +8% (Total = 35%)

