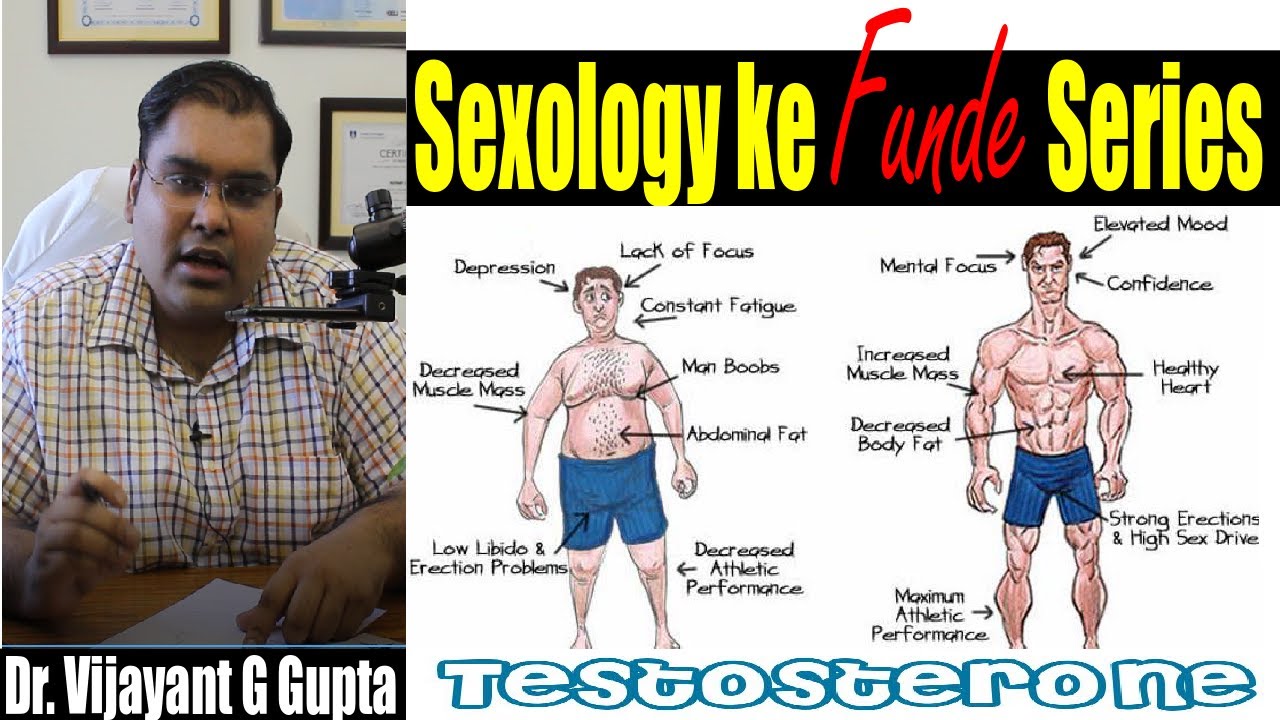
Testosterone Replacement Therapy (TRT) in India is a transformative treatment for men suffering from testosterone deficiency. While concerns about TRT-related risks exist, current scientific evidence overwhelmingly supports its benefits in improving quality of life, cardiovascular health, sexual function, and mental well-being.
At New Delhi Andrology Clinic, Dr. Vijayant Govinda Gupta offers expert consultation and customized TRT solutions to help men achieve optimal hormonal balance and health.
For consultations on TRT in India, book an appointment today with Dr. Vijayant Govinda Gupta.